How SNAP Cuts Are Threatening Food Is Medicine Programs — What Produce Prescription Officers Must Know Now
The Short Version
- H.R. 1's $187 billion in SNAP cuts removed 4.7 million people from food benefits since July 2025 — and the Boozman Farm Bill draft delivers zero restoration.
- Produce prescription programs face a structural vulnerability: their double-dollar farmers market model depends on an active SNAP participant pool that is now actively shrinking.
- Every $1 of SNAP spending generates $1.50–$1.80 in local economic activity — meaning cuts reduce the farmers market and food distribution ecosystem that FIM programs depend on, not just household purchasing power.
- States with CHCS FIM officers are best positioned to adapt: Section 1115 waiver-funded produce Rx creates a Medicaid floor that SNAP eligibility contractions cannot reach.
- FIM programs hold the outcome data a SNAP restoration coalition needs — connecting with FRAC and engaging the Farm Bill advocacy process is a natural extension of the state officer role, not a distraction from it.
July 4, 2025 was the effective date of the most consequential federal nutrition policy change in a generation. On that day, $187 billion in SNAP cuts signed into law under H.R. 1 began reshaping the food access landscape — quietly, without ceremony, while farmers markets were open and produce prescription vouchers were going out as usual. The infrastructure that Food Is Medicine programs depend on was already shifting underneath them.
For FIM state officers and Medicaid practitioners, what has unfolded since is a concrete operational problem. The people most likely to benefit from produce prescriptions are precisely those most exposed to SNAP cuts, and the June 23, 2026 Boozman Farm Bill draft — the vehicle many advocates hoped would provide relief — delivered none. This is a briefing on where things stand, why it matters for produce prescription programs specifically, and what FIM officers can act on now.
What H.R. 1 Did to SNAP — and Where Things Stand Now
What H.R. 1 Did to SNAP — and Where Things Stand Now
H.R. 1 achieved its $187 billion in SNAP cuts through three compounding mechanisms. It shifted program costs to states for the first time in the program's history, requiring states to fund a portion of benefits the federal government had always covered in full. It expanded work requirement time limits and eligibility restrictions, removing categories of currently-eligible adults from coverage. And it capped future benefit adjustments, slowing the inflation indexing that has historically kept SNAP benefits aligned with actual food costs.
The results have been rapid. According to the Food Research & Action Center, approximately 4.7 million people have lost access to SNAP since H.R. 1 went into effect on July 4, 2025. These are not people who left voluntarily — they are families and individuals who received benefits under prior rules and no longer qualify. The Congressional Budget Office has issued a longer-horizon warning: the CBO estimates some states will leave the SNAP program entirely due to the cost-shift structure.
Here is how the scale of that loss looks against the pre-H.R. 1 participation baseline, per USDA Food and Nutrition Service annual participation data and FRAC's count of those who have lost access:
SNAP's role as economic infrastructure helps explain why the ripple effects reach FIM programs well beyond directly affected households. FRAC's analysis of SNAP's ripple effects documents that every dollar of SNAP spending generates between $1.50 and $1.80 in economic activity — with the multiplier rising during economic downturns. That return flows into local food systems: farmers, processors, distributors, and the farmers markets where most produce prescription programs operate.
Contracting SNAP does not only reduce household food access. It reduces the economic foundation of the local food ecosystem that makes produce prescriptions viable in the first place.
Why the Boozman Farm Bill Draft Is Not a Relief Valve
Why the Boozman Farm Bill Draft Is Not a Relief Valve
The Senate Farm Bill draft released by Agriculture Committee Chair John Boozman on June 23, 2026 arrived with significant expectations from the nutrition policy community. For FIM advocates, the Farm Bill process had represented the most plausible near-term path to reversing or softening H.R. 1's SNAP provisions.
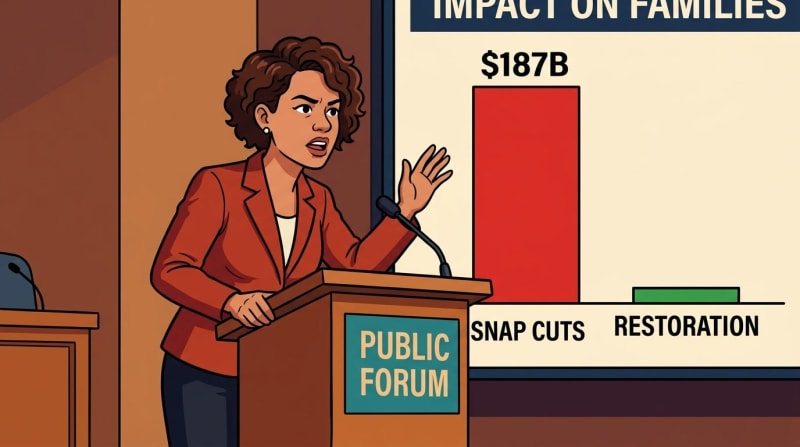
According to FRAC, the Boozman draft does not mitigate any of the $187 billion cut to SNAP enacted under H.R. 1. It does not restore the federal cost-share to its historic zero, roll back expanded time limits, or remove the benefit adjustment cap. For FIM programs that built participant pipeline assumptions around a stable SNAP baseline, this is a closed door — at least for the near term.
The gap between what H.R. 1 cut and what the Farm Bill restores is worth seeing in one frame:
FRAC president Crystal FitzSimons captured what that zero-restoration figure means for the communities FIM programs serve:
"By shifting program costs to states, expanding time limits, and putting a cap on future benefit adjustments, H.R. 1 has undermined SNAP, the stability of families, communities, and local economies, and weakened state budgets."
— Crystal FitzSimons, president, Food Research & Action Center, June 23, 2026
The state budget dimension of that statement matters particularly for Medicaid practitioners. The same cost-shift mechanism reducing SNAP participation is also constraining the state budgets that fund Medicaid innovation. A state absorbing new SNAP co-funding obligations has less fiscal room for Section 1115 waiver pilots, FIM program expansion, and medically tailored meal coverage. H.R. 1's impact is not additive — it compounds across programs that share a funding base.
The Farm Bill conference process is not over. Advocacy continues to matter, and the window for SNAP restoration has not permanently closed. But FIM state officers should not build near-term program operations around a legislative reversal that is not on the immediate horizon.
The SNAP-FIM Intersection: Why This Matters for Produce Prescription Programs

The SNAP-FIM Intersection: Why This Matters for Produce Prescription Programs
Food Is Medicine programs are designed to operate on top of an existing food access foundation — not to replace it. That foundation, in the United States, is SNAP. When SNAP contracts, FIM programs face a structural challenge their funding models were not built to address: absorb more unmet food need, or watch enrolled members' nutritional baseline erode.
The dependency runs deepest for produce prescription programs. FRAC documents that farmers markets depend on SNAP customers and on incentive programs — double-dollar matching, SNAP Market Bucks — that make fruits and vegetables affordable for low-income families. The produce prescription model most commonly operates through exactly this infrastructure: a SNAP-eligible member receives a produce Rx voucher, redeems it at a participating farmers market, and may stack it with a double-dollar match that multiplies the benefit.
When SNAP eligibility contracts, this model faces two simultaneous pressures. Fewer participants are SNAP-active, which reduces the double-dollar match pool that makes produce Rx financially viable for market operators. And members who lose SNAP face a steeper food insecurity burden — one the existing produce Rx benefit level was not calibrated to address alone.
The income-eligibility overlap between SNAP and Medicaid FIM programs illustrates why contraction in one directly affects the other. Under USDA SNAP rules, SNAP covers households up to 130% of the federal poverty level (gross income), with a 100% net income limit. ACA Medicaid expansion covers individuals up to 138% FPL — creating a narrow overlap zone where most FIM-enrolled Medicaid members are also SNAP-eligible. When H.R. 1 removes people from SNAP within this band, FIM programs lose their most natural participant population.
The CHCS FIM State Officer Program — funded by the Rockefeller Foundation and Builders Vision — places dedicated FIM officers in state agencies to advance Medicaid-covered FIM services. The conditions these programs address are food-system dependent: nutrition insecurity drives higher rates of diabetes, hypertension, and high-risk pregnancies, and contributes to health care costs that Medicaid bears disproportionately. The population FIM programs serve is the same population most exposed to H.R. 1's SNAP cuts.
States with active FIM officers carry a structural advantage in this environment — dedicated infrastructure, technical assistance, and a peer network for navigating exactly the funding contraction this brief describes. That is the gift available to states willing to move now, before enrollment attrition forces reactive decisions.
What does it mean for a produce prescription program to operate when the SNAP floor underneath it is actively dropping? That is not a rhetorical question. It is the operational question every FIM officer needs to answer with real enrollment data — not later, but now.
What FIM State Officers and Medicaid Payers Should Do Now

What FIM State Officers and Medicaid Payers Should Do Now
The first step is modeling. Every FIM state officer with a produce prescription program should run a SNAP overlap analysis: of your currently enrolled population, how many also receive SNAP? Of those, how many fall into the eligibility categories most affected by H.R. 1 — adults without dependents, individuals in states absorbing significant new SNAP co-funding obligations? That analysis translates the national 4.7 million figure into a program-specific enrollment attrition estimate you can actually plan around.
For programs with deep SNAP-linked participant populations, funding diversification is the structural response. Medicaid Section 1115 demonstration waivers are the most established path to produce Rx coverage that is not structurally dependent on SNAP participation. Several states engaged with the CHCS FIM State Officer Program have advanced or are advancing 1115 waivers that cover produce prescriptions as a Medicaid benefit. The waiver path is slower than SNAP-linked models, but it creates a Medicaid-funded floor that H.R. 1 cannot reach.
Medically Tailored Meals offer a second diversification path. MTM benefits funded through value-based care arrangements or managed care organization contracts carry less structural SNAP-dependency than produce Rx programs. For FIM officers serving members with the highest clinical complexity — advanced diabetes, heart failure, end-stage renal disease — MTM coverage may be the more durable near-term investment in a SNAP-constrained environment.
On advocacy: the Farm Bill conference process remains open, and FIM state officers hold standing that most policy stakeholders do not. FIM programs generate evidence — outcome data on produce prescription health effects, cost offsets, and food access gaps. That evidence is exactly what a SNAP restoration coalition needs to make a legislative case. Connecting with FRAC and the broader nutrition security advocacy network is not outside the lane of a FIM state officer. It is a natural extension of the role.
The families these programs serve did not create the policy environment they are navigating. They are people managing diet-related conditions with uncertain grocery access, families stretched by the loss of a benefit they counted on, communities where the gap between what people need and what they can afford was already real before H.R. 1 widened it. What FIM programs bring to those families — a produce voucher, a community health worker who shows up, a Medicaid benefit that treats food as care — matters more in a contracting SNAP environment, not less.
The policy landscape is harder right now. The need these programs address is not smaller. Those two facts point in the same direction: toward the work ahead, and toward the community of practice that makes it possible.
What would it mean for your program to become the bridge that holds when the SNAP floor drops? That is not a distant hypothetical. It is what the most resilient FIM programs are already building toward.
Content ID: WH8wMp7jJwmZW0uFegSMCOXU
See an error? Tell us.